
Re-visiting HART'S "Virus Model" Statement from 2023....
...and what I currently believe about 2020 and pandemics in general.

About 18 months ago HART (of which I am co-chair together with
) published the below article, which I will refer to hereinafter as the “HART Statement”:
Clare and I wrote that piece together. Because of some differences (even then) in certain viewpoints regarding the subject matter, it took some back and forth regarding the wording to come to a version we both found acceptable.
However, during the past 18 months, as a result of my own research, deliberations and evolving thought processes, I feel it is now necessary to distance myself from the position taken in that article as I no longer agree with most of what was written there.
Now, it is true that HART - like any organisation - is made up of a broad church of people with various overlapping but non-identical opinions.
However, most of HART’S articles to date have been published without being attributed to individual authors, which gives the impression that what is presented is a viewpoint shared by all its members.
Clearly, as people’s knowledge and opinions evolve, deviations will arise between what people wrote (or allowed to be written and published on their behalf) and what their current beliefs are, and it is neither sensible nor practical to continuously point all these out as they arise.
However, the subject matter of the above particular article is so central to my own beliefs about what happened in 2020 and what needs to happen going forward that I feel the need to create some sort of statement to which I can point people who misunderstand or misrepresent my own beliefs about the subject matter discussed.
This current article is in 2 parts:
Part A is about specific issues I now have with what the Hart Statement states - either explicitly or by implication.
Part B outlines my current thinking as regards the nature of the event called “the covid pandemic” and pandemics in general.
This article is not intended to provide all my detailed reasoning for the positions I hold; it is, rather, intended to be a statement as to what I currently believe, augmented by links to just a few of the many key relevant articles I have written or co-authored.
If you want to dig deeper into why I hold the beliefs I do, then peruse the many articles at the following locations.
My own substack:

Articles co-authored with others at:



A. Problems with the HART Statement.
1. No single, defined model for what a virus is either structurally or functionally.
The title assumes there is an actual definable single verifiable “virus model” which explains how some infectious diseases spread and make people ill.
The subtitle - Arguments against "the virus doesn’t exist” - sets the article up somewhat as a straw man exercise.
What I mean by the above is that it suggests that if you don’t accept “the virus model” (whatever that is) you are automatically in the category of those who say “viruses don’t exist”.
Yet, I don’t regard these as mutually exclusive categories.
To explain further: the definition of “viruses” cannot be divorced from the functional characteristics generally assumed to be attributed to them.
I made this point on X a few months ago - click here or on the picture below to go to the tweet itself, where you can also see the foregoing debate which led me to chip in to the discussion:
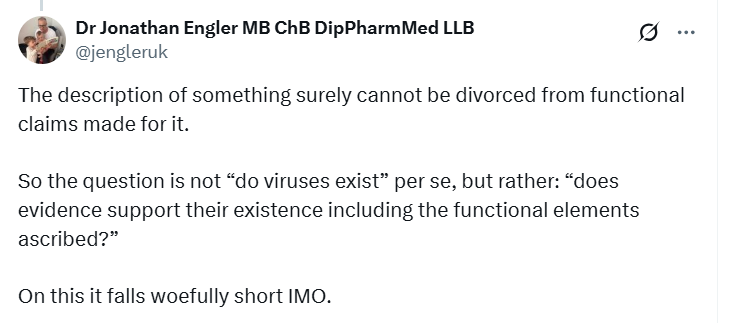
Put another way, if “viruses” are defined by reference to the generally accepted model of contagion, person-to-person transmission, immunity, herd immunity and so on, then - in relation to respiratory illnesses at least, then no, I do not think they exist.
This is not the same as denying that there are “things” which can be detected by “tests” more often when people are ill than when they are well. I accept that this does seem to be the case, though it doesn’t seem at all clear what those “things” are or what the “tests” are actually measuring. But it is a huge leap from that observation to accepting the generally accepted models of contagion as they relate to what are termed respiratory viral infections (and which underpin “pandemic” theory”); in my view, these are built on sand.
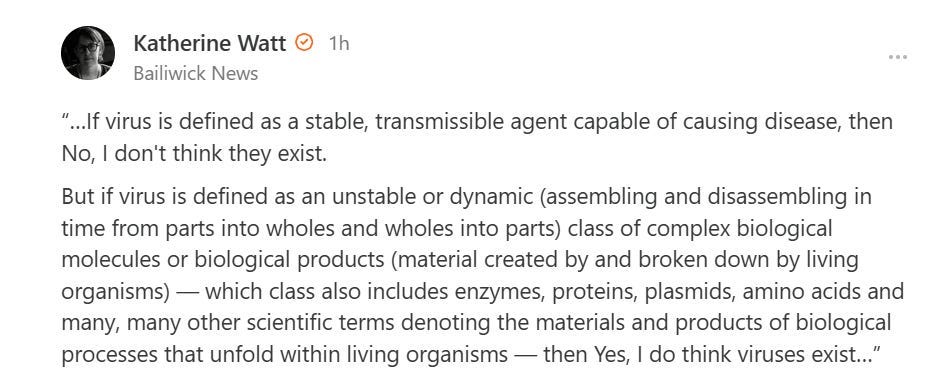
I would agree with the way Katherine Watt puts it here:
2. Failure to replicate transmission.
I am not going to repeat what has been well-described elsewhere, but in short, in my view the failure - observed in attempt after attempt - to replicate the transmission of respiratory illness between “infected” and well persons using methodology apparently optimized for the purpose is fatal to the model generally assumed to be operational.
“Can you Catch a Cold” by Daniel Roytas contains a thorough exposition of the history of such experimentation. His conclusions regarding the specific studies he references which I have read do hold up.
3. Invalidity of the one-to-one pathogen-illness relationship.
The HART Statement (and other articles written under the HART banner) suggest that illnesses of the type called “covid” can be linked to an individual virus, and that through various tests the “spread” of that virus can be tracked.
I reject those assertions.
For one thing, whenever attempts have been made to identify the pathogens responsible for respiratory illnesses, the finding of a single, identifiable pathogen is not the norm. More often, no pathogen, or multiple pathogens, are found.
For more on this, see in particular this recent article:

The pandemicists rely on the story that “covid wiped the flu out” to counter the accusation that “covid was flu rebranded” - since there was no real increase in spring 2020 in people attending hospitals with respiratory illnesses, as would be expected if a new contagious and deadly respiratory virus was rapidly circulating.
As I described here, in order for “covid” to have wiped out the flu (a fantasy story which is dismantled by this series of articles which demonstrate that this is a testing rather than a biologically-driven phenomenon), it would have to have also wiped out all the other causes of “influenza-like illnesses”; this is an even more fantastic story than one in which just one purported cause is wiped out.
Moreover, pre-2020 doubts that swabbing the nose or throat had any relevance to illnesses thought to be associated with pathogens in the lungs just seem to have been ignored, yet this would seem to be a further fatal or near-fatal flaw in the establishment pandemic narrative, as I wrote here a year ago:
4. No novel pathogen in 2020.
In my view there was no change in 2020 to the environment in terms of the “virome” - whatever that actually is! Instead, tests were rolled out which “found” “something” which caused those tests to light up positive, but that “something” had been present for some time. In fact, “it” had found its way across several continents completely unnoticed until the WHO implored everyone to “test, test, test”.
The contortions the pandemicists resort to in explaining how something so contagious and deadly can behave in that way are wondrous to behold, but there’s a serious point to be made here about burden of proof.
To me, adherence to the scientific precept of “parsimony” (whereby the simplest explanation is the default hypothesis which must be disproven) demands that the burden is on the “pandemicists” to explain how and why something so contagious and deadly can spread such that - by use of the same tests as used later to “track the virus” - it has been encountered by more than half the population without causing any clusters of unusual illness or excess deaths. This is what happened in New York, as I wrote here:
New York - it was widespread well before anyone noticed.

Jessica Hockett Martin Neil and I have written a lot about the paucity of evidence for the official pandemic narrative.
As yet, no such explanation has been forthcoming.
Use of the phrase “this virus” in the article strongly suggests that a new pathogen came onto the scene. I do not believe that happened. As I have stated elsewhere, “the pandemic” was - in my view - constructed using these ingredients:
Propaganda
Targeted dystopian hospital and care home policies
Fraudulent testing
Data fraud
Notably, the “recipe” did not and does not require a new pathogen. I say more on the practical significance of this below.
5. Testing alone can create the illusion of novelty and spread, and did so in 2020
The article suggests that antibody measurements and sequencing outputs support the “novel spreading virus” theory.
Again, I reject these assertions. These tests are not - in themselves - proof of a novel spreading pathogen. I am not going to be expansive here on why, but I have written or co-authored many articles on this.
In brief, I believe that the fact that the original PCR test was developed without access to clinical material from anyone with “the disease”, based on a sequence for “the virus” built in silico using clinical material apparently obtained from someone with an illness indistinguishable from other illnesses assumed to be “respiratory viral” conditions is extremely problematic for the validity of all the tests developed later and which, for THEIR validation, were dependent on that test, (which included later PCR tests, rapid antigen testing and serology.
I touch on the circularity of this here:

For a description of some of the problems in relation to sequencing - inasmuch as it supports the idea that a novel virus spread round the world - I recommend the work of Ben at
.This article of Ben’s - and the comments under it - are particularly worthwhile reading; while doing so, recall that every single diagnostic test - be it PCR, Rapid Antigen tests, or seroprevalence measurements - ultimately relies on the fidelity of “the sequence”:

Finally, it’s worth emphasising that the mistaken illusion of an epidemic created and driven by testing is certainly NOT a new or previously unknown phenomenon, as I wrote here:
False positive PCR-driven pseudo-epidemics are nothing new - they happen all the time.

I naively keep making the assumption that people know the stuff I have known for ages, so apologies if this is all “old news” to you.
6. No novel disease in 2020
People claim - and the HART article implies - that “covid was different”. Yet, in reality the symptoms of “covid” were so overlapping with the symptoms of other “influenza like illnesses” that the claim that there was a novel disease cannot be substantiated.
It is worth restating what I touched upon above: there is not one article written before spring 2020 (when the “emergency” came into being”) describing any clusters of unusual illness caused by this “unique, deadly and contagious virus” - despite substantial and now unchallenged evidence that “it” had become widely distributed across several continents by that time. In my view, this strongly implies that all the purported differences between “covid” and other respiratory illnesses are explainable by a combination of observation and confirmation bias, and things which were done differently to people in the face of “suspected covid”, whether or not supported by “a positive test”.
Martin Neil has published a number of pieces on the substack he shares with Norman Fenton, some of which I co-authored) digging into the literature on the clinical characteristics of “covid” compared to other respiratory illnesses. Suffice to say, the novelty trope does not appear to be well-founded.
The best article to read in this respect would be this:
B. What are pandemics and what happened in 2020?
The HART Statement discussed in part A does not explicitly cover this broad-ranging question, but having addressed my issues with that, it seems opportune to state my position about the events of 2020 clearly for the record.
The points I make below are accepted by many “covid dissidents”, but frequently such acceptance will be caveated with something like “it was still different” or “it was nasty because it was man-made”, or “those phenomena only explain part of what happened”; as will be seen below, I reject these assertions and maintain that all the events of the last 5 years can be explained without the need for a novel virus to have emerged, whether from Wuhan or anywhere else.
1. Modern-day pandemics are not biological phenomena
I believe that pandemics are socio-political events, not biological phenomena.
It is - to my mind - no coincidence that the plethora of “pandemics” or “near pandemics” (SARS, H1N1, MERS etc) declared in the 21st century coincides with the widespread adoption of new sequencing-based technologies used for “virus hunting”.
In other words, it’s a phenomenon caused by looking for - and finding things - which are already there, and then reacting to them.
I like the exoplanets analogy in this regard. Exoplanets are planets circulating around stars other than our own sun. Before the existence of exoplanets was first confirmed in the 1990s, their existence was entirely theoretical. Now, wherever space telescopes are pointed in the sky, exoplanets can be detected orbiting the stars observed.
Nobody would argue that these exoplanets are new, nor that any new threat by way of alien invasion has come about. It’s only the discovery that is new.
Even the “Spanish Flu” pandemic narrative would appear to be full of holes, which I am not going to go into here, other than to remark that I don’t think it is coincidental that it followed a period of massive societal and political disruption, horrendous suffering, malnutrition, population relocation as well as medical experimentation. The idea (as has been claimed) that a respiratory virus actually targets and disproportionately kills young males - rather than this being the demographic sent to be slaughtered during WW1 - is almost comical if it weren’t so tragic. It has certainly been useful for political leaders, both as an explanation for the deaths of so many, and also for the need for governments “to be prepared”.
Finally, I would note that the underlying assumption, which seems to be being pushed by the WHO and other proponents of “pandemic preparedness” that “pandemics are increasingly likely” would - on any simplistic logical basis - appear to be the opposite of the truth.
Firstly, rising living standards lead to increasingly well-nourished societies with better access to clean water, which reduce vulnerabilities to infectious diseases, making “pandemics” inherently less likely.
Secondly, increased population mixing and travel - by spreading “immune memory” more widely over the globe - should theoretically reduce rather than increase the chance of pandemics. (I should point out that I am here using the established model - which I should emphasise I don’t accept - against those who claim an ever-increasing risk from pandemics).
2. Nocebo effects are important but misunderstood and rarely considered.
I have written fairly extensively on this topic - see the articles here.
Again, I am not going to repeat what I have already said other than by way of summary. In brief:
The placebo effect is the positive effect on symptoms from something given with the expectation that it will make the recipient better.
The nocebo effect is the deleterious effect on symptoms and well-being caused by something done which creates an expectation that the person will either (1) become ill when they were previously well, or (2) will become more ill than they were before.
It must be remembered that in 2020 and beyond, the establishment bombarded us with the most intense, sophisticated and longest propaganda campaign ever waged on humanity. I believe we have hugely underestimated the extent of the physical symptoms induced thereby.
Notably, it is well-recognized that breathlessness can be induced by nocebo effects - see here, or here by way of example.
It should also be borne in mind that propaganda inducing nocebo effects would combine synergistically with social media augmented by the internet, especially where any countervailing viewpoints were being suppressed.
3. The wet-market vs lab-origin “debate” is “permitted discourse” but a false dichotomy.
I first realised that the perpetrators didn’t really care about this issue in 2022, as I wrote here:
This is the key quote from that article:
I don't think we are asking the right questions about Spring 2020 at all. Timing of "lockdown" is quite obviously a distraction from the core issue. But I also think natural vs lab origin is not the most pressing question to answer.
To me, the way "lab-leak" was initially verboten, yet now seems to be permissible to talk (and write) about has a smell of being “managed”.
If I imagine that the major part of the mortality had been caused by a variety of policy decisions I had made, the number one thing I'd want is for people to occupy themselves obsessing over the origin of the virus rather than the cause of the deaths.
Imagine that I was heavily involved in the "pandemic preparedness industry" - an industry siphoning billions out of the pockets of taxpayers into my chosen commercial interests. I wouldn’t be bothered about the origin story. Lab or natural - I can make a fortune either way.
What I would be bothered about though would be the idea that this was in fact nowhere near as harmful as the "authorities" told people it was. Because then people might question the need for my new highly profitable industry at all.
I could even tolerate people thinking it was a lab leak. If it was, people will be afraid that it could surely happen again. Because regardless of whatever controls are put in place, some rogue operators could always carelessly carry on doing GoF research.
So natural or lab-leak, as long as we keep the fear going, we surely need to be better "prepared". That's great for business. And great for justifying centralised control.
Since then, together with Jessica Hockett, we have come to understand that false binaries have played an important role in steering the narrative and keeping debate within “permitted” tramlines, the idea that there was no novel pathogen causing a pandemic being well and truly OUTSIDE those lines.
In this regard it is well worth reading this piece, which lists more such “false binaries”:

4. “Gain of Function” is really “Claim of Function”.
One of the main arguments advanced by those who claim that a novel virus spread round the world causing a novel illness, is that “scientists were conducting gain of function research in Wuhan”.
To that I would say “so what?”
For one thing, just because something was said to have been found in Wuhan first, it doesn’t mean that that is where it originated. Great Barrington Declaration author Sunetra Gupta agrees with me on this.
If one set out to peddle a false narrative about a novel virus originating or escaping from a certain location then it would only be natural to choose somewhere with some credible tenuous connection to “a lab”. Alternatively the idea that “it” originated there could have emerged organically because a lab was located there and because (as has been stated) there was a history of poor biosecurity and hence people were watching it closely.
As it so happens, the story of what happened in China would appear to be as full of holes as the description of what happened elsewhere, as Thomas Verduyn wrote here.
But my main objection is actually that there is no proof that scientists can create pathogens with pandemic potential, and just because someone may have been trying to do so, it doesn’t mean it happened. When the evidence is actually looked at in detail, it is extraordinarily scanty.
Martin Neil and I wrote extensively about why we think “gain of function” would be more aptly called “claimed of function”; links to a short-form version of our article can be found here, and the full version here.
In any event, in relation to the “hypothesis” of a “lab-leak”, it is remarkable how vague such a theory is, given it is promoted as a “case-closed” explanation of the entirety of “the pandemic”. As Jessica Hockett writes here, for such a hypothesis to have any real explanatory power, it really needs to contain some semblance of exactly what happened, when and how, rather than merely “somehow, it must have escaped”.
5. Official data stories and narratives are not to be trusted.
I am frequently asked “so what happened in Northern Italy, or New York, then?”
To be clear, notwithstanding that I have no doubt that people died through the dystopian policies enacted during spring 2020, I regard the mortality curves claimed for those events - and probably similar events in other locations - as unsubstantiated and fraudulent in magnitude, timing or both. In other words, those are staged events which would have required substantial coordination and pre-planning to pull off.
For Bergamo,
and I explain why here. For NYC, this is one of the many articles Jessica has written on the topic.Nobody has really explained how and why a purported pathogen can have no discernible effect in one area, but be responsible for a mass casualty event in another nearby locale.
For the spring 2020 New York City event it is claimed that a 9/11’s worth of deaths happened every week for about 2 months. Yet - as explained in the article referenced above - despite being in an age when every citizen can (and frequently does) pull out their phone to make and post their own short video clips - there is no footprint of the massive and unprecedented body management efforts which would have been required.
What’s worse, nobody seems interested in investigating. If the data is NOT fraudulent, citizens should be demanding to know why so many people died in such a short period of time - ie what precisely was so wrong with “the response” and who is responsible for what happened?
Alternatively, if the deaths did not happen at the times or in the numbers claimed, people deserve to know how, why and by whom this deception was carried out.
Yet, all we have is silence, combined with the imbecilic acceptance that “NYC was hit hard”.
6. There was much iatrogenic harm in 2020 (which continues to this day)
Notwithstanding that some mortality curves appear fraudulent, I do not deny that some people died (all labelled, of course, by the authorities as “covid”) who otherwise would not have died in spring 2020, creating (in some places) some episodes of excess death.
However, there is substantial evidence that these additional deaths were caused by a variety of dystopian protocols imposed on hospitals and care homes.
These span isolation, neglect, maltreatment, nontreatment and mistreatment, including protocols which amount to euthanasia, as I document extensively below:
It is notable that these deaths commence upon the rollout of the “emergency response”, not having occurred anywhere beforehand, despite evidence (according to the “official” tests later used by officials to measure such things) of spread of the purported pathogen for months beforehand.
Summary of Parts A and B:
The above parts can be summarised by stating clearly what I do NOT believe, which is the following:
Respiratory viral illnesses spread from person to person.
A new pathogen came on the scene in 2020 whether from a wet-market, a laboratory or elsewhere.
Scientists can create or modify viruses (wherever they are) so as to endow them with pandemic potential.
Pandemics - as generally understood by that word - can occur in healthy populations.
It follows from the above that I regard virology as a discipline built on foundations of quicksand.
I am not going to say more on this here as I don’t think it’s necessary, other than to mention that my doubts extend to all of vaccinology as well - which is to a large extent dependent on the validity of models derived from the principles of virology.
It’s worth pointing out here that I have harboured these doubts for some time, and I regret not making my position clearer at an earlier stage, although notably, a year ago (as HART) Clare and I did co-author this article which casts doubt on the “vaccination eliminated smallpox from the face of the earth” trope - a claim which forms the centrepiece of the praise bestowed upon vaccinology.
Concluding remarks: why does any of this matter?
I am frequently asked why this all matters, as long as we are all working together and towards showing that there was an “overreaction”, and getting the products known as covid vaccines taken off the market.
My answer is that we must never - explicitly or by implication - accept the idea that there was anything which actually required any sort of response at all.
The reason for this is that if I am right, the perpetrators can repeat the exercise (with improvements from the “lessons learned”) at any time of their choosing.
All they need to simulate the appearance of a new spreading threat is a story or rumour of some “lab leak”, some propaganda and a fraudulent test rolled out at breakneck speed.
It is important to realise that this is not just a theoretical, hypothetical worst-case scenario. It is actually what appears to be happening (although whether or not this develops into another full-blown “pandemic emergency” remains to be seen):
Our worst fears are coming true.

Quick post to point out this substack note, and the associated developing story:
One major concern I have about the present “we must ban gain of function” discourse is that even if it is “banned”, methods to stage pandemics are still available:
firstly, a claimed new and staged pandemic could be portrayed as “zoonotic” in origin
secondly, a story that a rogue state or non-state actor has caused “a lab leak” would be incredibly easy to plant, notwithstanding that such research was banned.
No doubt this new leak will be of a more deadly virus than “covid” because “the scientists have learned from their mistakes”.
So it should be easy to see how this threat could just hang around like a sword of damocles.
As regards challenging the “covid vaccines” and related mandates, whilst this is important, it cannot be seen as the be all and end all of fighting the madness we see before us.
As
put it here: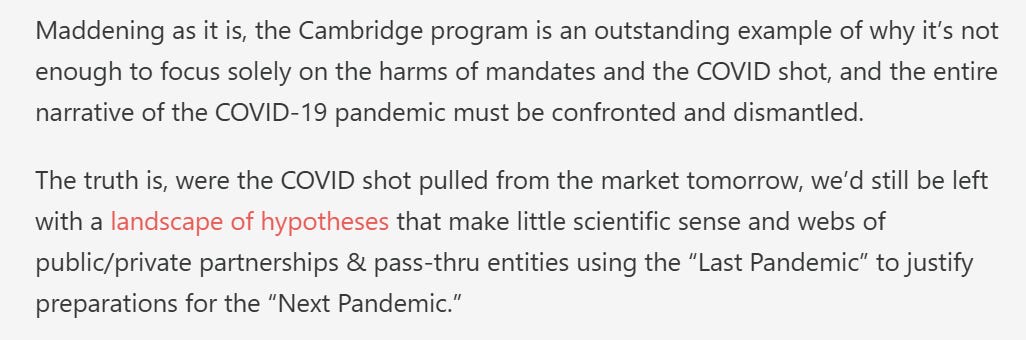
(As I wrote here, the Cambridge Programme mentioned refers to Cambridge University’s new “Engineered Pandemics Risk Management Programme” - supported by a £5.25m grant from someone whose identity we are not allowed to know.)
It is clear that those who profited so handsomely over the past few years have no intention of giving up.
They want “pandemic preparedness” to be a permanent global agenda item.
Fighting this entails demonstrating all the ridiculousness, lies, corruption and fraud associated with the event known as the “covid pandemic”.
Very thought provoking article that has a distinct ring of truth, unlike most of the official narratives we have been force-fed for years. My trust in politicians, the medical profession, the regulatory authorities, the pharmaceutical industry, billionaire philanthropists, main stream, medical and scientific media has been shaken to the core. As a retired doctor I have had to revisit all of my medical training and assumptions and question everything. Thank you, and others at HART, and all those writing in the alternative media for providing so much food for thought. Your efforts have been much appreciated.
It's pretty amazing how despite the evidence to the contrary, many still cling onto their "scientific" fairy tales.
The viral theory of disease is a crazy idea that invaders somehow hack our cells to copy themselves. They're dead but somehow alive. Sounds like fantasy to me!
Then there's this super complicated genius immune system that even they cannot figure out. Why? Because it's not that complicated, it's a garbage collection system!
https://robc137.substack.com/p/fix-the-foundation-before-the-roof
https://barn0346.substack.com/p/life-is-not-a-battle
The rest of germ theory also falls apart when considering basic ideas. Bacteria only feed on dead matter. Right now there's strep A in your throat and e-coli in your digestive system and guess what, you're not infected right now. Hmmm 🤔