
Now here's a real pandemic...
Well, not really. Not in the contagious pathogen sense.

I - like many of us - have become well aware of increasing numbers of people receiving antidepressant medication and other drugs for all manner of psychiatric illnesses.
I was curious to see what proportion of adults were on such drugs. The actual numbers reported for depression (the most commonly diagnosed mental illness) are astonishing.
According to statista, in 2023 17.8% of American adults currently had or were being treated for depression, up from 13.5% in 2017

This article is from 2016 - I am sure the number will be higher now.

In the UK, usage is also startling. According to this1 BBC News article “from 2021-22, there was a 5% rise in the number of adults receiving antidepressants - from 7.9 million in the previous 12 months to 8.3 million” (out of a UK adult population of around 60 million).
When I posted the US data above on X, someone responded as follows:

The “umbrella review” referred to is this. It is published in Molecular Psychiatry, part of the Nature stable of journals, and is open access. The lead author is:
I must admit that, despite me having become cynical about most pharmaceutical products (especially the “blockbuster” drugs like statins and SSRIs), this particular story passed me by. But it is a truly astonishing one, because what the authors conclude following a huge systematic review is this:
The main areas of serotonin research provide no consistent evidence of there being an association between serotonin and depression, and no support for the hypothesis that depression is caused by lowered serotonin activity or concentrations. Some evidence was consistent with the possibility that long-term antidepressant use reduces serotonin concentration.
Nearly all antidepressants prescribed today (by market size) are selective serotonin reuptake inhibitors - SSRIs.
As this report points out, the market is huge and growing fast.
The global antidepressants drugs market was valued at USD 17.02 billion in 2022 and growing at a CAGR of 7.90% from 2023 to 2032. The market is expected to reach USD 36.41 billion by 2032.
It probably doesn’t need stating that the underlying basis for their use is the theory that depression is linked to serotonin levels in the brain being too low, and that by blocking (“inhibiting”) its reuptake by nerve cells after messaging, more serotonin is available to pass further messages between nearby nerve cells.
However, this paper demolishes the evidence base for that2. From the discussion:
This review suggests that the huge research effort based on the serotonin hypothesis has not produced convincing evidence of a biochemical basis to depression. This is consistent with research on many other biological markers [21].
We suggest it is time to acknowledge that the serotonin theory of depression is not empirically substantiated.
So, how exactly was this paper received? Well, what you might have learned from the past few years is this:
The pharma and biotech industries are huge and very powerful
They heavily influence all scientific publishing and mainstream media
They have bought all notable “opinion leaders”
So it might not surprise you to learn that the paper sustained attack upon publication, and immediately so - it was published on 20 July 2022 and this compendium of critical comments appeared the same day on the website Science Media Centre, which suggests that they were alerted by the publisher (Nature) to procure such comments before the publication date.
Science Media Centre is in itself an interesting creation. It was originally formed in 2002 as a division of the Royal Institution of Great Britain. It is a registered charity with the following objects:

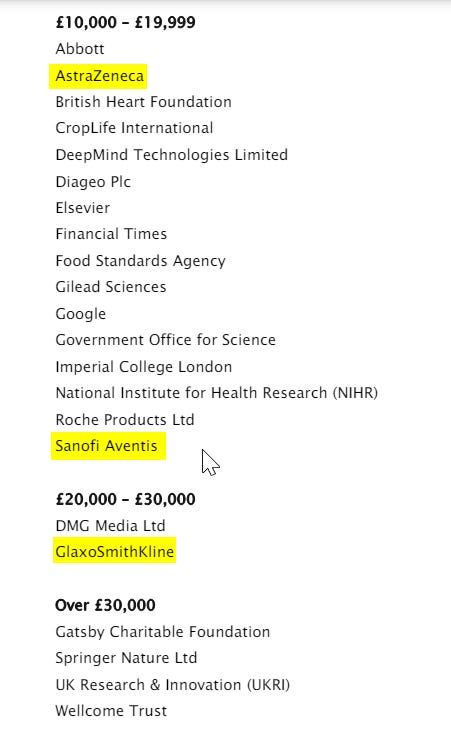
Accounts for the year ending 31 Mar 2023 (the year in which the events above occurred) can be found here.
These are the largest donors in that year - the highlighted ones are the top 3 in the antidepressant market:
The authors responded - quite credibly in my view - however the pharma-industrial complex fought back in familiar style - by trashing the lead author in a popular mainstream publication - in this instance Rolling Stone:

Many of the talking points in this article are the predictable and now familiar slurs by association, lazy characterisation of opinion as a “right-wing” phenomenon, and straw man tropes:
It was “promoted extensively by far-right commentator and professional transphobe Matt Walsh”..
Tucker Carlson spoke about the study on his show.
Moncrieff has spent years actively questioning the efficacy of SSRIs and the nature of mental illness in general, as well as promoting widely disputed beliefs about the dangers of various mental health interventions such as antidepressants or alternative forms of treatment.
…the review was largely met with yawns from the psychiatric community. “In reading it, I was kinda thinking, ‘Wow, next she’ll tackle the discrediting of the black bile theory of depression,”
Moncrieff cites pediatric vaccine mandates in the United States as an example of the “paternalism” of public health interventions,
More recently, she has used her platform to publicly question mandatory Covid vaccines for health care workers in the U.K.. Last year, she was one of the signatories of an open letter from health care professionals opposed to the mandates, which, while acknowledging that they can be helpful for some people, maintained “there is considerable uncertainty about the effectiveness of the Covid vaccines.”
In speaking about the dangers of SSRIs, Moncrieff has dabbled in the same vein of light conspiratorial thinking that characterizes her views on vaccines.
The responses to Moncrieff’s seratonin / SSRI critique can be summarised thus:
It’s old news and trite observation that the mechanisms of depression are more complicated than just being about serotonin.
BUT it’s irrelevant anyway because the trials show that SSRIs work so well.
But do they really?
To address this, I would suggest reading the rebuttal the authors wrote (also referenced above), especially the section specifically addressing this point.
It won’t surprise you to read that:
Meta-analyses show that the benefits of SSRIs over placebo are paper-thin in practical terms - the old relative versus absolute benefits issue.
Such purported benefits could be explained by methodological issues in relation to the conduct of the studies. Specifically, the benefit of the active drug over placebo is so slim that any enhanced placebo effect (from patients knowing from side effects that they were in the active group) could account for all the difference observed3.
Trials supporting SSRIs are usually short - weeks or a few months - whereas treatment is generally for years or lifelong.
Trials are sponsored by the manufacturers, and whilst this has been the norm for decades, the past few years should have taught us to be very wary of this conflict of interest, especially since regulators appear to no longer do much actual regulating.
Moncrieff cites these two papers as recent criticisms of antidepressant trials:
This paper4 published, in the BMJ in 2019, was a reanalysis performed by the Nordic Cochrane Centre of a major earlier systematic review. Having found that “Several methodological limitations in the evidence base of antidepressants were either unrecognised or underestimated in the systematic review by Cipriani et al.” it concluded as follows:
The evidence does not support definitive conclusions regarding the benefits of antidepressants for depression in adults. It is unclear whether antidepressants are more efficacious than placebo.
For this article (published in BMJ’s Evidence Based Medicine) the authors performed a systematic review targeting narrative and systematic reviews with the search terms ‘depression’ and ‘antidepressants’ published between 1990 and 2019; they concluded:
The benefits of antidepressants seem to be minimal and possibly without any importance to the average patient with major depressive disorder. Antidepressants should not be used for adults with major depressive disorder before valid evidence has shown that the potential beneficial effects outweigh the harmful effects.
Of systematic reviews, which attempt to integrate all the published evidence for a scientific proposition to come to a single authoritative conclusion, it must be remembered that publication bias5 will have a huge effect on what evidence is found.
Hence it must be concluded that the evidence base for one of the most lucrative drug classes in history would appear to be somewhere between weak and non-existent.
And we haven’t even got onto adverse effects, one the most disturbing of which is sexual dysfunction. As this essay suggests, this is underdiagnosed, can persist after stopping treatment, and is often attributed (wrongly) to the recurrence of depression:

Interestingly, that BBC news article also contains the pharma promotion headline “Anti-depressants work, major study says” linking to a 2018 news item reporting on this Lancet study. About this it states “Scientists say they have settled one of medicine's biggest debates after a huge study found that anti-depressants work”. So “the science is settled” didn’t start with “covid” by any means. As you will read further down in this article, a reanalysis by the Cochrane Centre in Denmark came to the opposite conclusion.
It even suggests that longer-term it could make things worse: “Some evidence was consistent with the possibility that long-term antidepressant use reduces serotonin concentration.”
This fascinating trial is referenced, in which “patients were all given an antidepressant, but half told that it was a placebo and half told the truth, those who were been told that they had received an antidepressant showed twice the change in anxiety and depression scores compared to those who believed they had received the placebo”.
This is the reanalysis referred to in footnote 1.
The propensity for studies which do not find the result desired by those funding the research (nearly all drug trials are paid for by the manufacturer) to be forgotten about and never published, significantly biasing the published evidence base in favour of the desired finding. See here for a good description.
I'd recommend...
"The Emperor's New Drugs ( exploding the antidepressant myth )" by Irving Kirsch.
If memory serves it quotes meta-analysis on the efficacy of SSRIs.
And maybe...
"The Medicalisation of Every Day Life" by Thomas Szasz
I was convinced ( I say convinced because at the time it was obvious that these pills would help me, anyone knew this to be true, how could one know better !) to take SSRIs for a short period, my reaction to them got me thinking about what they were, I stopped and this experience partially factored into my reaction to covid vaccines, as in, 'get that shite away from me' and 'why would recommend this to me, are you sociopathic, deluded, apathetic, all of the above?'
I pretty much came to the conclusion that there are little resources available for people to deal with problems in living on personal human levels.
So conveniently people are shunted onto these lucrative pills, doctors get you out of their office, money is made, family feel like you are doing something, you feel like you are doing something, because no-one really knows at that point what's wrong, or where to turn, we don't have reference points, and it's frightening.
So what better target, times of existential vulnerability, multiplied by billions of people, by thousands of pills, off which to make a killing. Now that's a model plenty of CEOs could get behind.
SSRIs are based on a false premise, the serotonin model, it doesnt hold up well !
Was it ever believed by the creators, probably a mixed bag there.
Many [ forms ] of depression are cyclical, there's a 'regression to the mean' that occurs, this could make it appear like the drugs are effective over these periods. How many other pharma products' efficacy partially hide behind this statistical reality.
There does seem to be a placebo effect, it makes sense from what we know of this phenomenon, a cohort of people will feel improved by taking, if they believe in them!
In retrospect my own doctor, I suspect, had this stance, that they might help through placebo, he also recommended talk therapy, what else could he do, but this method has to be unethical, no?
So similarly to the vaccines, I believe, we have a mutifold veiled 'effect', backed by censorship and marketing of a hugely resourceful industry, aided by regulatory capture, and the usual assortment of theories as to what the doctors are about.
Brain chemistry could obviously come into play, but the mind could affect this clearly in return, so show the cause / effect there's a good scientist ( good luck with that ! ), this 'cure' has not shown much efficacy, a cursory dive should convince that it cannot address the complexities involved here, given its supposed mechanism of action.
And all that is without even looking at the harms, physical and psychological.
Anyway, maybe preaching to the choir here, but encourage anyone wondering to check out that book for a primer on counter arguments, and try decide if you should, although your life won't necessarily be any better by not taking them of course...
ok heavy bias 😂
Well done, Jonathan. I have said this, multiple times, on multiple 'stacks. One of my happiest outcomes from the Great Covid Debacle is the number of people coming out (of the woodwork) and/or "getting religion" regarding how completely and irredeemably chock-full of crap are the drug companies. Covid wasn't the first example of the rot. Hell, it might not even be the best. (I have a personal feeling that Phen-Fen, at least in the U.S., was one of the finest examples of the types of B.S. that passes for safety oversight from the FDA.) It seems to me that one could establish a rule-of-thumb stating, "If Big Pharma is making a ton of money off a drug, that drug is garbage, along with any ostensible proof offered during its approval process." I admit to being a little strident!