
"Covid" euthanasia protocols and the UK's infamous "Liverpool Care Pathway"

This was one of my most widely read pieces:

It details the evidence that specific hospital and care home protocols were implemented which effectively euthanised people who “tested positive for covid”.
In that, I give evidence pertaining to a number of countries, while focussing on the UK.
My firmly-held conclusion can be gleaned from the title of that article:
The rapid rollout of testing and euthanasia protocols was used to create the appearance of a sudden-spreading deadly novel virus.
In the UK, the main evidence for the use of midazolam and opiates resulting in premature death comes in the form of the NICE guideline NG163. For more, see these specific numbered sections of my article as linked above:
16 - intro to NG 163 including the instititutional support for - and some against - it
17 - Official Scottish Covid Inquiry hears evidence consistent with its widespread use
18 - excess deaths in UK closely track midazolam doses used
23 - Official Scottish Covid Inquiry hears evidence consistent with zero informed consent for applying “do not resuscitate” orders
25 - detailed analysis of the wording of NG163
Of course, NG163 wasn’t the UK’s first rodeo in terms of a scandal involving euthanising patients using sedative drugs, as Andrew Bridgen pointed out yestoday on X:

What was the LCP?
In 2012 a huge story broke in the mainstream press in the UK - the “Liverpool Care Pathway” scandal - click the picture below to go to an archived version of the below Telegraph article on it.

That article explains that the majority of NHS trusts in England received financial rewards for placing terminally ill patients on the “Liverpool Care Pathway”. Payouts totaling over £12 million were linked to meeting specific targets, such as the number of patients on the protocol.
The LCP, designed to ease suffering by withdrawing unnecessary treatments, faced backlash amid claims it was used to hasten death without family consultation.
A review followed (“independent”, of course) led by Baroness Julia Neuberger, and a report - “More Care, Less Pathway” - was published in July 2013.
The below bullet points summarising the key findings and recommendations in the report are generated with the assitance of Gemini AI:
Key Findings
Poor Implementation and Clinical Care: While the LCP works well when used by trained, sensitive teams, it was frequently used as a “tick-box exercise” by staff who were poorly trained or rushed.
Failures in Communication: Relatives often felt “railroaded” into decisions, were not told their loved ones were dying, or discovered dramatic changes in treatment (like sedation) without any prior discussion.
Concerns Over Hydration and Nutrition: There was significant distress caused by the “inhumane” withholding of oral fluids from thirsty patients and a misunderstanding by staff that the LCP meant food and drink must be withdrawn.
Misuse as a Protocol: The LCP was often misinterpreted as a set of instructions (a protocol) to be followed blindly rather than a flexible guideline, leading to inappropriate sedation and a failure to recognize when a patient’s condition might be reversible.
Lack of Accountability and Oversight: Families often did not know who was in charge of a patient’s care, particularly during nights and weekends when senior staff were absent and specialist palliative care was unavailable.
Key Recommendations
Abandon the “Pathway” Terminology: The name “Liverpool Care Pathway” should be replaced within 6–12 months by an individualized “end of life care plan” to remove the “conveyor belt to death” association.
Ensure 24/7 Specialist Access: Funding must be made available so that specialist palliative care teams are accessible for advice and hands-on support 24 hours a day, seven days a week, in both hospitals and the community.
End Financial Incentives: Local financial incentives (CQUINs) that paid hospitals based on the number of patients placed on the LCP must cease to prevent the perception that deaths were being hastened for profit.
Mandatory Training and Competence: All clinicians caring for the dying must demonstrate proficiency in communication and symptom management as part of their professional revalidation and induction.
Clear Accountability and Documentation: Every dying patient must have a named senior responsible clinician (Consultant or GP) and a named nurse for every shift to ensure clear lines of responsibility and better communication with families.
How similar were the LCP and NG163?
Again, I used Gemini AI to do a comparison. There was no single document summarising the LCP protocol, so I asked Gemini to use these three sources:
LCP Generic Version 12 (Official Template): Detailed workflow and symptom checklists.
Thames Valley Cancer Alliance Palliative Guidelines: A common example of the local guidelines used to implement LCP-style prescribing.
Neuberger Review (More Care, Less Pathway): The independent report that led to the pathway’s withdrawal, citing concerns over “tick-box” applications of these dosages.
For NG163, I found a copy of the actual protocol online and Gemini used this in its analysis:
Here’s the output. The table below and similarities / differences bullet points are all generated by Gemini:
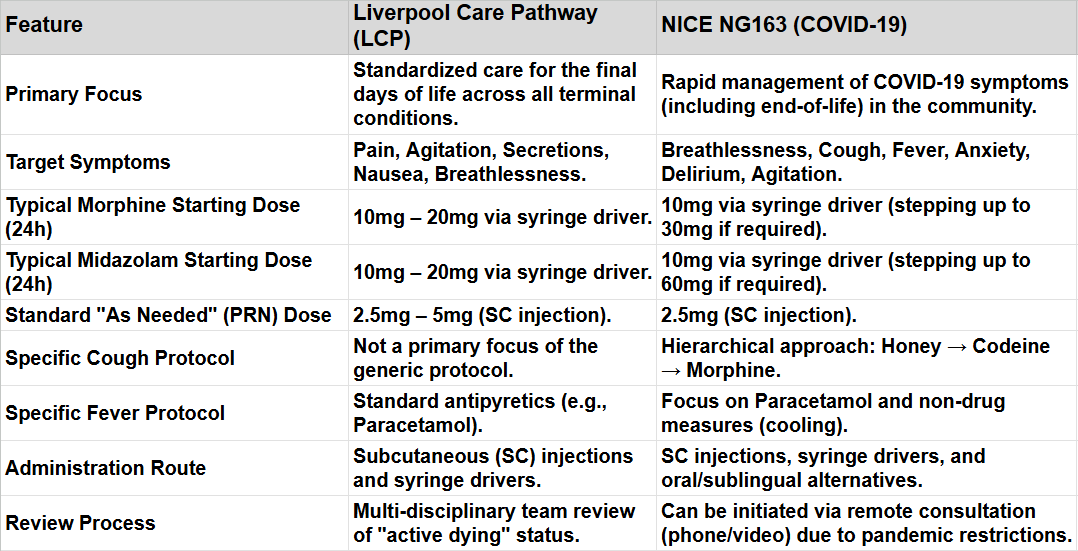
Essential Similarities
Anticipatory Prescribing: Both protocols advocate for prescribing “just in case” medications to ensure there is no delay in treating distressing symptoms at the end of life.
Core Medication Duo: Both rely heavily on the combination of an opioid (Morphine) and a benzodiazepine (Midazolam) to manage the common “terminal triad” of pain, breathlessness, and agitation.
Subcutaneous Delivery: Both utilize subcutaneous injections and continuous infusions (syringe drivers) as the preferred method when a patient can no longer swallow.
Symptom Titration: Both frameworks emphasize starting with a low dose and increasing it based on the patient’s clinical response rather than a fixed maximum.
Essential Differences
Symptom Specificity: NG163 contains unique instructions for COVID-specific symptoms like a dry, distressing cough and high fever, which were not detailed in the generic LCP.
Consultation Method: The LCP required frequent bedside assessments. In contrast, NG163 was designed for a pandemic context, explicitly allowing for remote assessments to manage patients in the community.
Breathlessness Management: While both use Morphine for breathlessness, NG163 provides more specific “step-up” advice for severe COVID-related respiratory distress, including the use of Lorazepam or Haloperidol alongside Midazolam.
Context of Application: The LCP was (supposedly) a comprehensive “pathway” covering nutrition, hydration, and spiritual care; NG163 is primarily a “symptom management” guideline focused on pharmacological interventions.
Conclusion:
These protocols clearly share a common ancestor - if not actually via documents, certainly via an ideology.
I recommend readers who simply cannot believe that healthcare professionals ever cross ethical boundaries familiarise themselves with this article:
When it comes to the vast majority of healthcare "professionals," I don't believe they have any ethical boundaries to cross. In 2020 they proved themselves to be sociopaths almost to a man, either actively participating in evil or approving of it through their silence. Whether you believe their medical errors kill 100,000 Americans every year or four times that, the fact that the trend is never downward, and that they aren't up in arms about the horror of it all, says everything you need to know about their ethics.
It makes good sense to say they must have done this.
https://baldmichael.substack.com/p/care-homes-and-midazolam-the-murder?utm_source=publication-search